Young Matt and I spent about 6 hours in the cadaver lab on Saturday afternoon.
I am forever fascinated by human anatomy, and it’s always a learning experience no matter how many times I get in the lab.
By the way, I’ll be teaching an cadaver anatomy course in the fall for PT’s in a virtual palace of a facility in the fall. More on that later.
Our goals for Saturday’s lab time was to dissect out all the peripheral extremity nerves in preparation for attending NOI Group’s Mobilization of the Nervous System Course next week.
Here’s some highlights and clinical thoughts from the lab…
We dissected out the shoulder with the goal of following the suprascapular nerve. First and foremost, in looking at the infraspinatus… not a single trigger point in sight! 🙂
The nerve is easy to find at the suprascapular notch under the superior transverse scapular ligament. As you follow it around the lateral aspect of the spine of the scapula it goes deep where it supplies the infraspinatus with a number of branches. If you reflect back the entire infraspinatus to expose the infraspinous fossa, you can get a good look at the branching of the nerve.
Clinical thoughts: If you have a client with posterior shoulder pain, a loss of shoulder internal rotation, or horizontal adduction, you may want to take a look at this nerve. The sensory branches are more prolific than you think. Considering the possibilities of neurogenic inflammation and mechanosensitivity as a result of injury to the target tissues or surgery, you have to consider the need to treat not only the tissues but consider the state of the nerve itself. Here’s my buddy Zac Cupples performing the neurodynamic test for the suprascapular nerve.
[Click on the photos to enlarge them]

Image courtesy of Visible Body (www.visiblebody.com)
In the lower extremity, we looked closely at several nerves that influence symptoms in common knee and ankle injuries.
We followed the saphenous nerve from the adductor canal. Our main focus here was to follow the infrapatellar branches that are implicated in a number of knee issues.
Clinical Thoughts: Post-surgical conditions, Knee contusions, MCL sprains, and general knee sensitivity in kneeling warrants assessment of the saphenous nerve as it is frequently irritated. If you ever had a client complain of anterior or medial knee soreness or pain long after typical tissue healing time, be sure to take a look at this nerve. Remember that the typical saphenous neurodynamic test is done with the knee extended. To differentiate the infrapatellar branches requires knee flexion to bring them under tension.

Image courtesy of Visible Body (www.visiblebody.com)
We went to the distal posterior thigh to identify the split in the sciatic nerve into the tibial nerve and common fibular (peroneal) nerve. Young Matt went to work on the deep and superficial branches of the common fibular nerve, and I worked on uncovering the sural nerve. We were able to expose and identify them all the way to their distal locations in the foot.
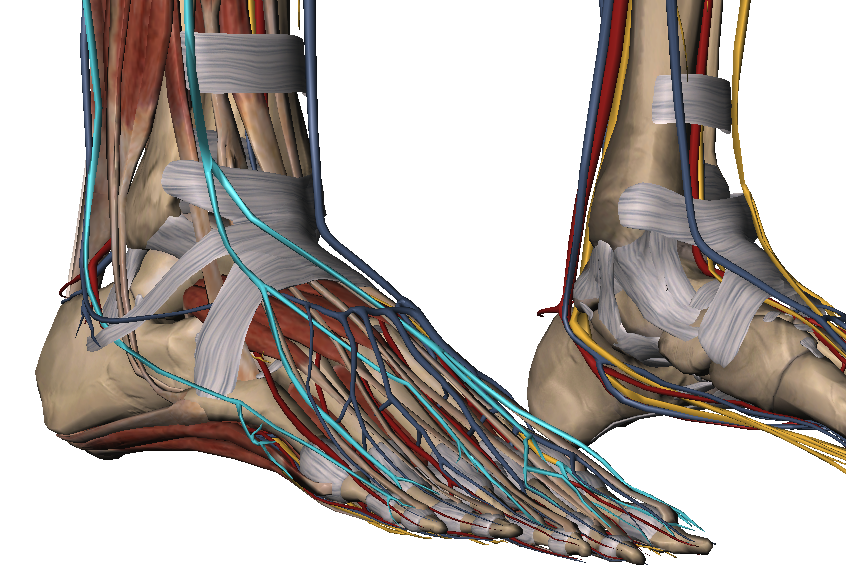
Image courtesy of Visible Body (www.visiblebody.com)
Clinical Thoughts: The superficial fibular and sural nerves deserve special attention in any form of lateral ankle injuries like an inversion sprain, foot contusions, or any form of ankle surgery. Their coverage of the lateral ankle and dorsum of the foot is quite broad. You can tweak them with small modifications to your straight leg raise test. Here’s Zac again showing proper execution of the neurodynamic tests.
Overall, it was a very solid day in the cadaver lab with many more to come.
Be sure to sign up for the newsletter as subscribers will be the first to get word on when the cadaver anatomy course will take place this fall.
Recommended Resources


